Quantitative LC-MRM (multiple reaction monitoring) methods for small molecule drugs are used to provide bioanalytical support in various stages of drug discovery and development. These methods can routinely achieve lower limits of quantification (LLOQ) in the range of 50 to 100 pg/mL, in various biological matrices, using analytical-scale chromatography (e.g., 2.1 mm I.D. UPLC Columns). In the case of peptide therapeutics, these assays are more challenging because lower LLOQs are often required.
One method that allows significant sensitivity enhancements is to operate the LC-MS system at lower LC flow rates, which provides reduced chromatographic peak volumes and increased ionization efficiency with electrospray ionization mass spectrometry (ESI-MS). However, most “homemade” capillary-flow LC-MS configurations suffer from a lack of robustness and are often not able to provide adequate sample throughput. The ionKey/MS System is an integrated capillary-flow microfluidic system that is designed to operate in the flow range of 1 to 5 µL/min, which can provide a 10- to 20-fold increase in sensitivity for therapeutic peptides when compared to conventional analytical-scale LC-MS platforms.
Oxytocin (OT) is a mammalian, 9-amino-acid cyclic peptide (CYIQNCPLG-NH2) that acts primarily as a neurotransmitter in the brain. Quantitative measurement of endogenous OT in biological samples is very challenging, because it is present at low pg/ml concentrations in human plasma.1 ELISA2-3 and mass spectrometry assays3-6 have been previously reported for measurement of endogenous OT levels. However, the LLOQ of commercial ELISA assays for OT is above the endogenous level. Several methods using mass spectrometry have been developed recently using affinity capture for OT enrichment,3 two-dimensional (2D) LC-MS/MS using a tandem quadrupole MS in conjunction with large-volume sample extraction (1.4 mL human plasma),4 or 2D-LC-MS/MS with large volume injection5 to achieve the required sensitivity.
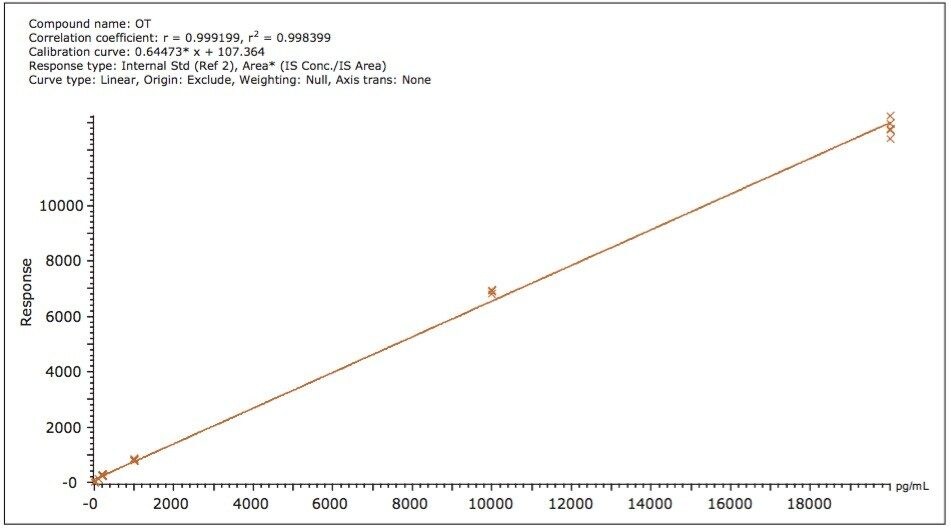
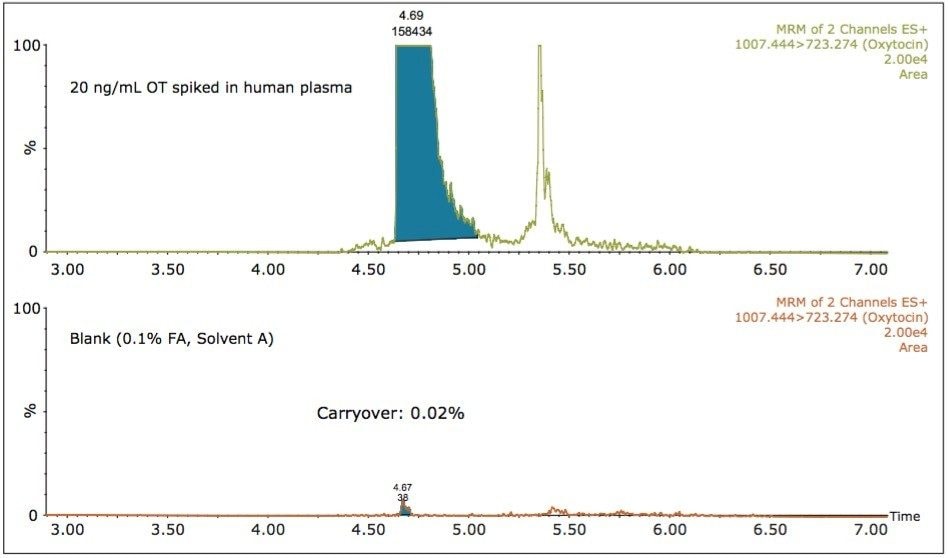
Here we report an LC-MRM method developed on the ionKey/MS System that is able to detect very low levels of OT in human plasma, at an LLOQ of 10 pg/mL.