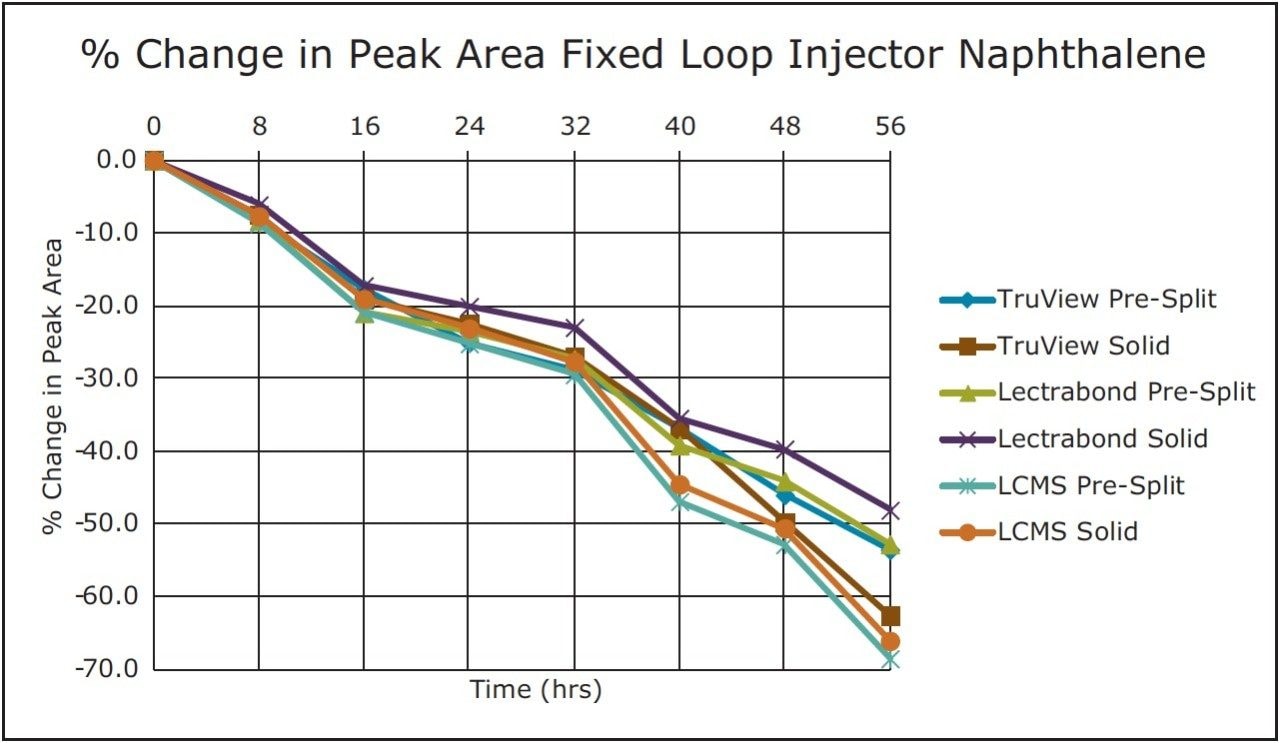
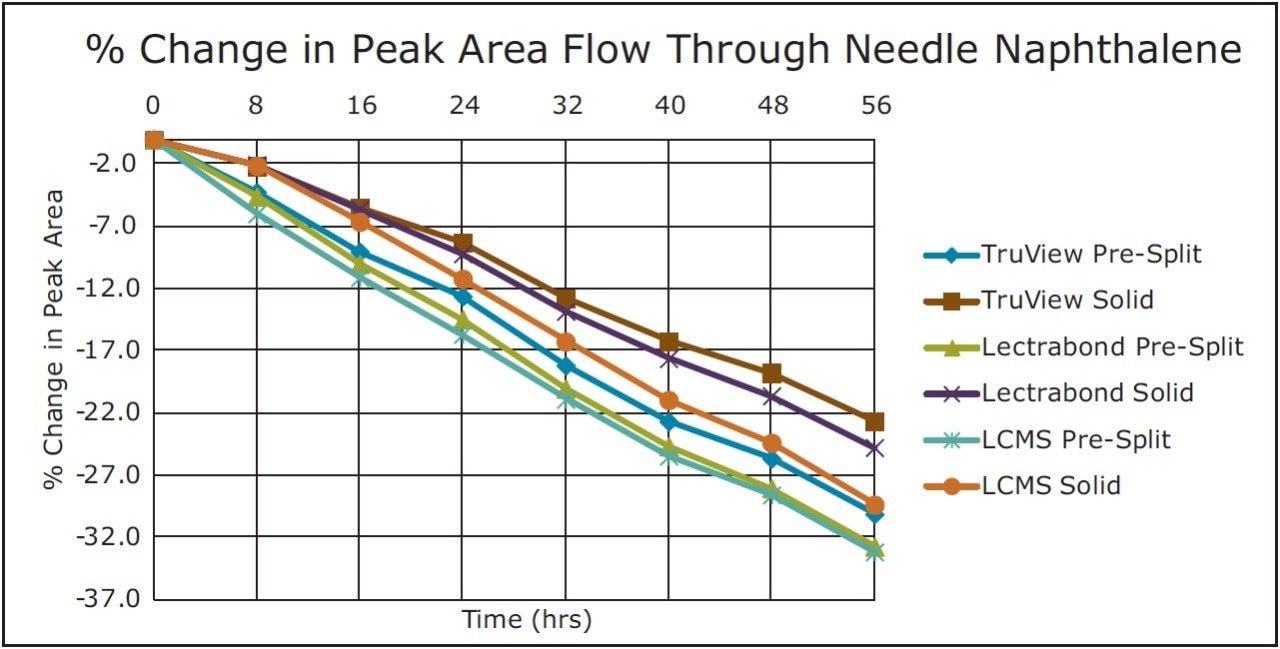
For the volatile compound naphthalene, the analyte evaporation component again dominated though the changes were about half that observed with the fixed loop injector. As above, none of these caps prevented the significant change in concentration for this analyte over the study timeframe.
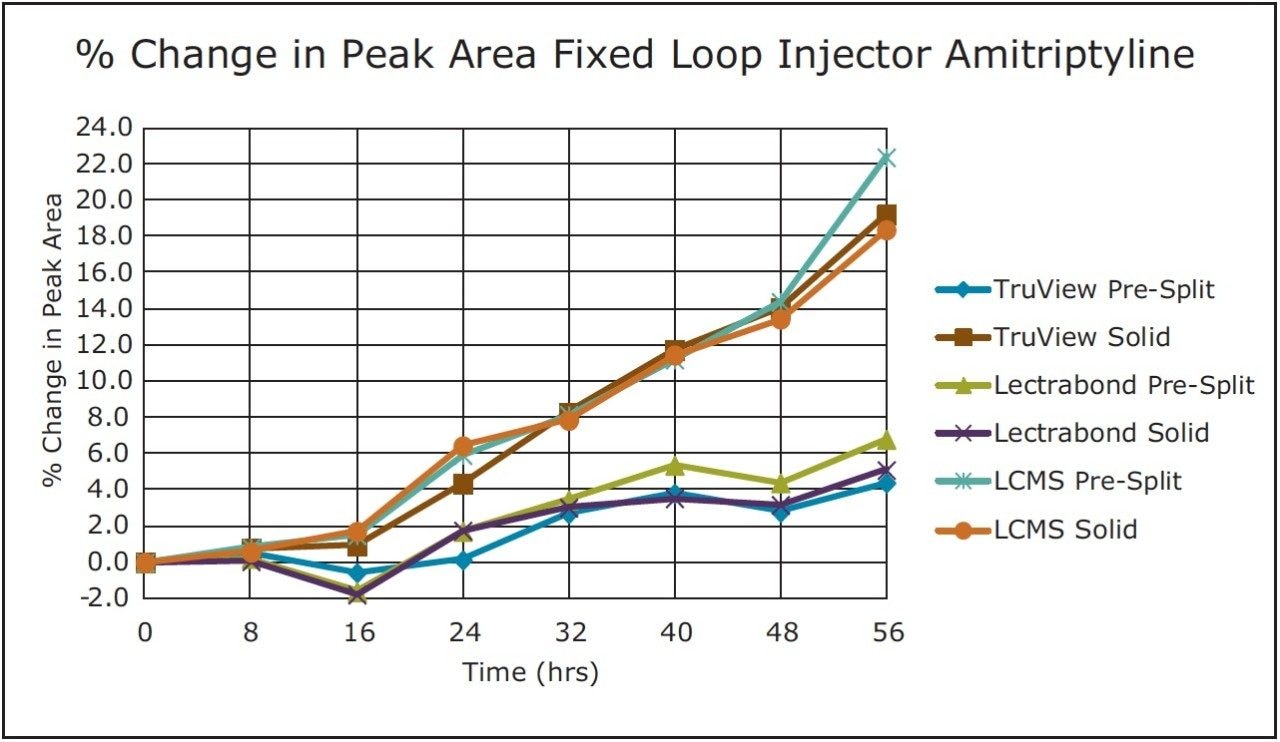
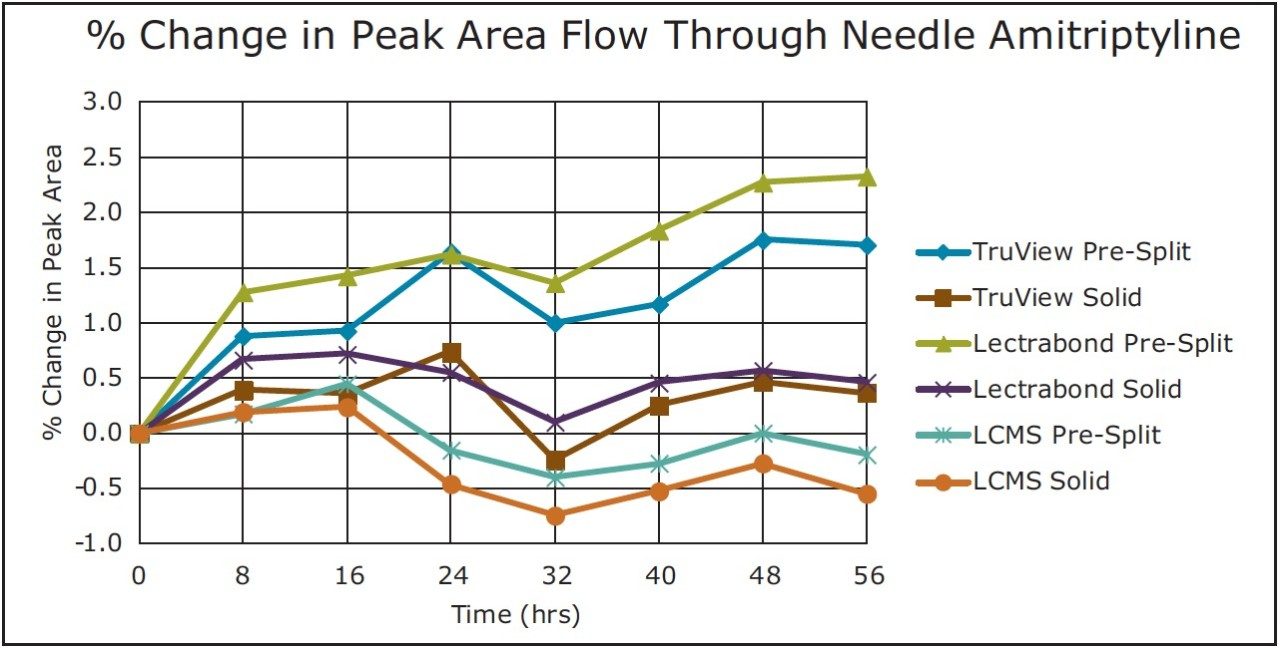
For the non-volatile compound amitriptyline, there were only small changes in this analyte concentration via diluent evaporation. With the lower % peak area changes (TruView Solid, Lectrabond Solid, LCMS Pre-Split, LCMS Solid), there is some fluctuation in the data suggesting those changes may be within experimental sampling error. All the tested vial cap types resealed sufficiently to keep the % peak area change in the -1% to +3% range over the study timeframe.
The differences in results between the fixed loop injector and the flow through needle Injector (FTN) are due to the disparity in outside diameters of the septum piercing these injectors make (OD of 1.83 mm vs. 1.00 mm, resp.). The smaller flow through needle Injector (FTN) piercing allows for a better reseal after each injection. However, when good control over volatile analyte concentration is desired, the results suggest that frequent cap septa changes are advisable, regardless of the injector and cap type used.
For non-volatile analytes with a volatile diluent, the results depended on the injector used. With the fixed loop injector, the TruView Pre-Slit, Lectrabond pre-split and Lectrabond Solid septa gave better resealibility across the multiple injections and longer time periods. For the flow through needle Injector (FTN), there was much less difference among the different septa, with the TrueView Solid, Lectrabond Solid, LCMS Pre-Split and LCMS Solid septa performing best.