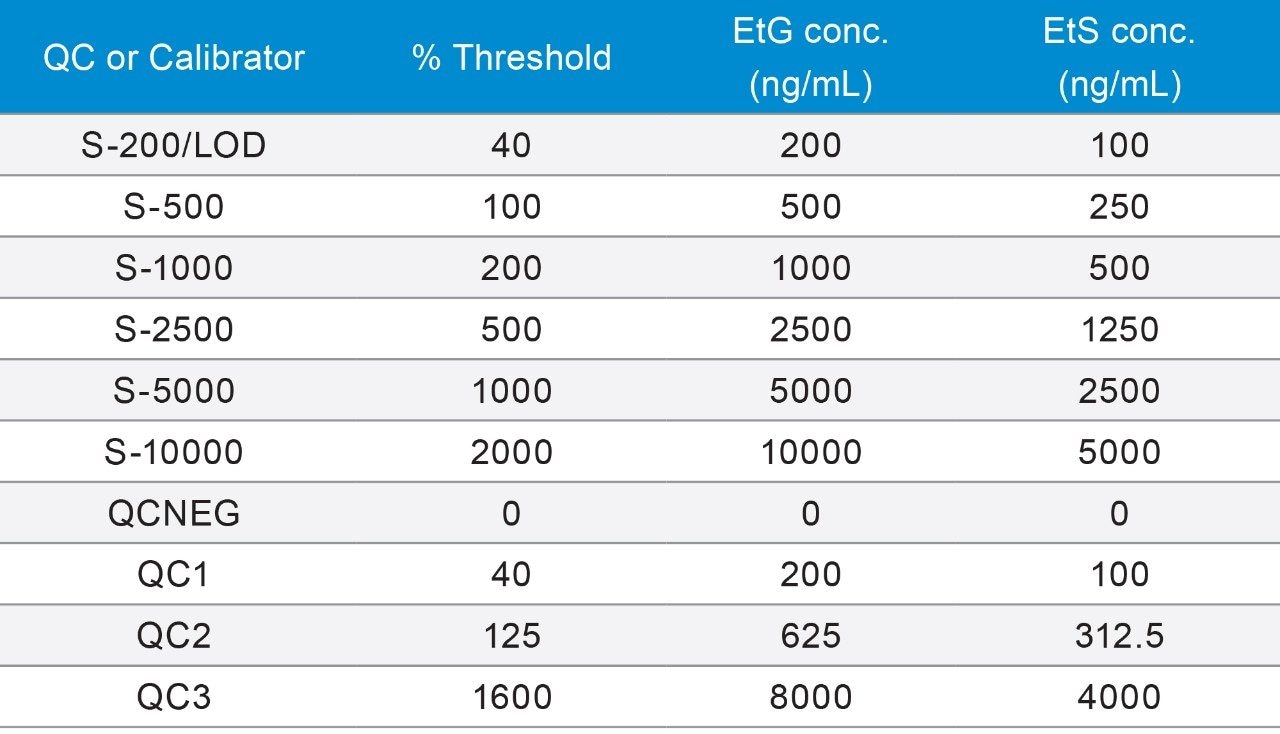
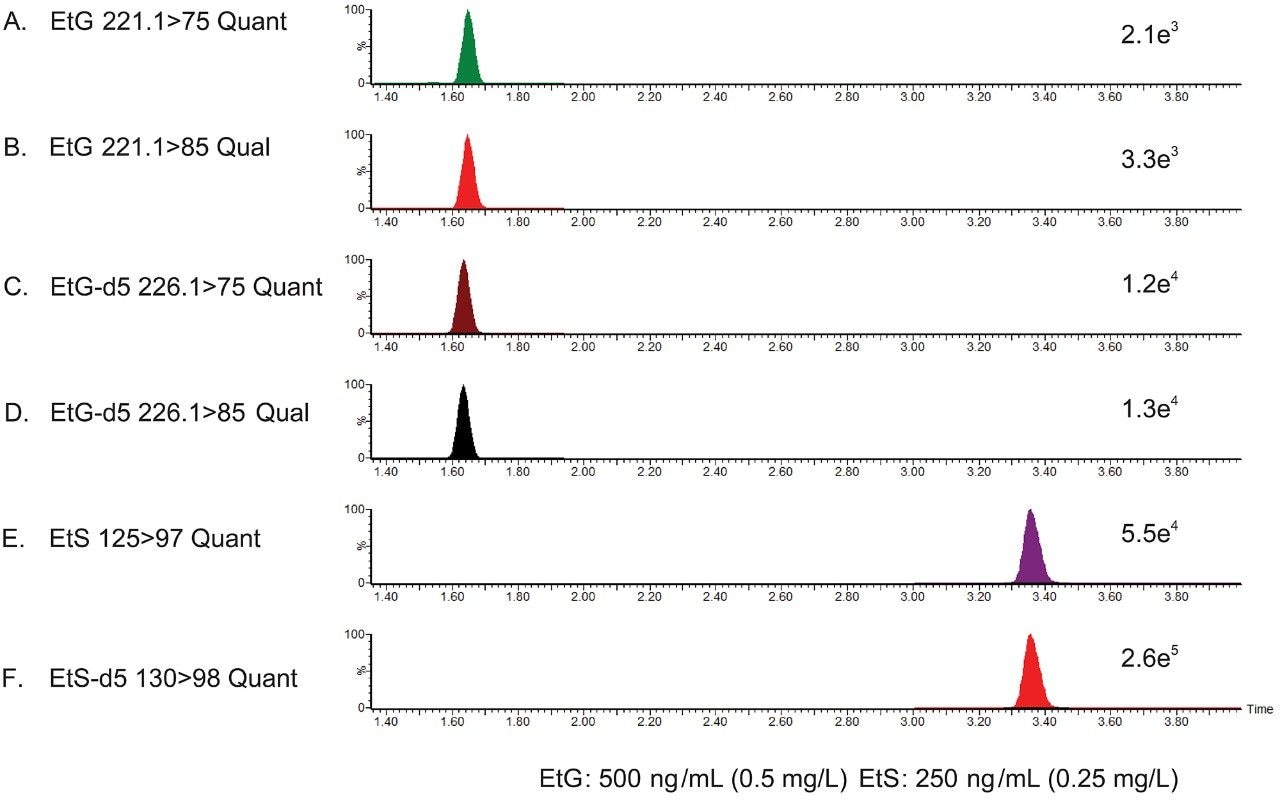
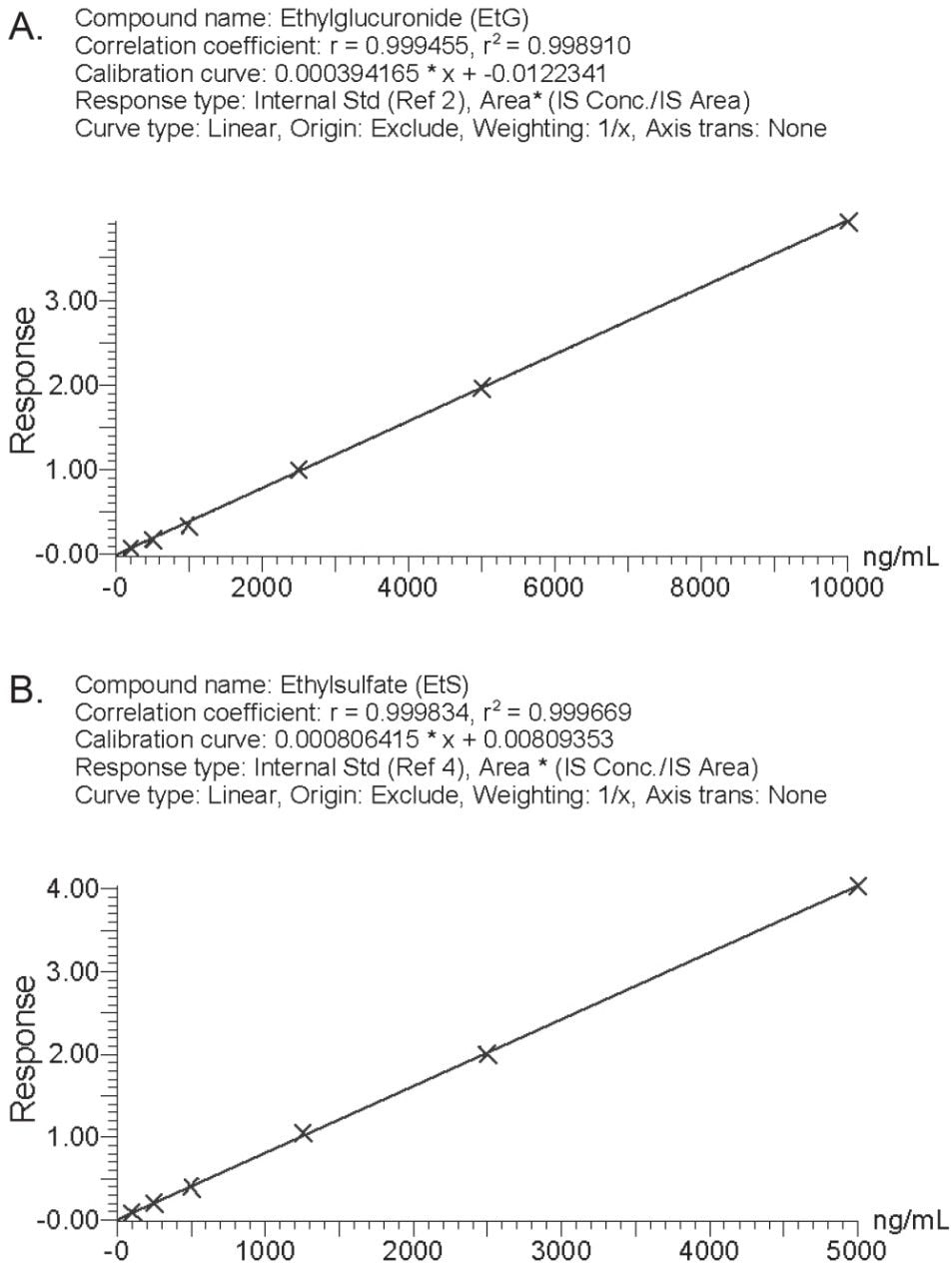
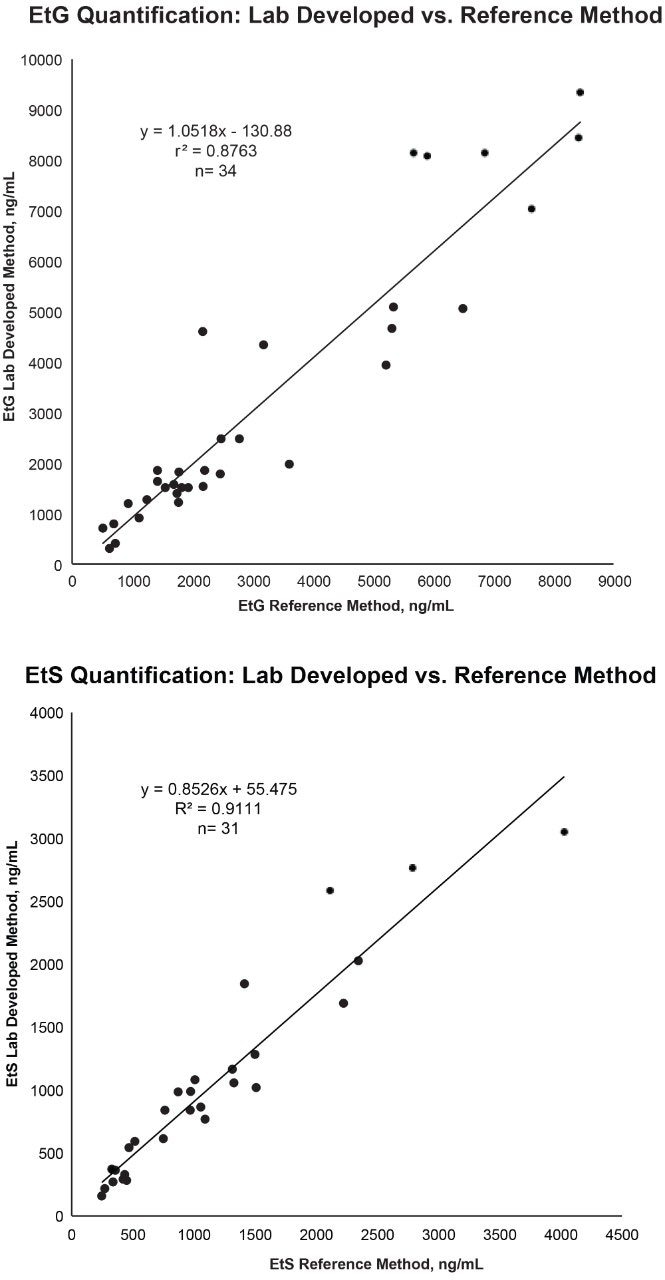
Calibration curves were generated based on the ratio of the response of the analyte’s quantifier ion relative to the response of the quantifier ion for the respective deuterated internal standard. Regression lines were plotted using a 1/x weighting. Calibration curves for EtG (r2 range: 0.991–0.999) and EtS (r2 range: 0.997–0.999) were linear over the analytical ranges investigated, and extended from 200 to 10,000 ng/mL and 100 to 5,000 ng/mL for EtG and EtS, respectively (Figure 2). The cut-off for the assay was set at 500 ng/mL for EtG and 250 ng/mL for EtS. The limits of detection (LOD) were determined using the lowest non-zero calibrator approach. LOD’s for EtG and EtS were set at 200 ng/mL and EtS 100 ng/mL, respectively.
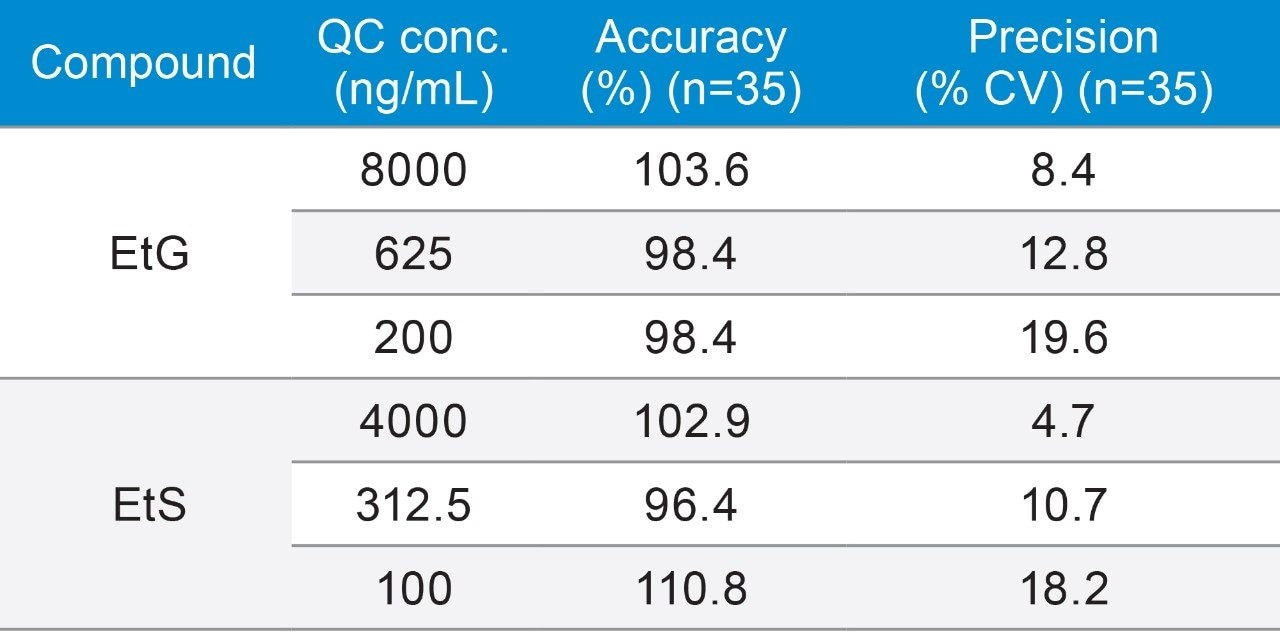
The precision and accuracy of the method were assessed at three QC concentrations for EtG (200, 625, 8000 ng/mL) and EtS (100, 312.5, 4000 ng/mL). Based on 11 analytical runs, consisting of three or four replicates, the assay precision (%CV) and accuracy for EtG ranged from 8.4 to 19.6, and 98.4% to 103.6%, respectively. The assay precision and accuracy for EtS ranged from 4.7 to 18.2, and 96.4 to 110.8%, respectively. In all, the method showed good precision and accuracy as summarized in Table 4.