Tumor Necrosis Factor (TNF) is a vital protein that plays a key role in the regulation of immune response. Therefore, biotherapeutic TNF inhibitors have been used to great effect in the treatment of inflammation diseases such as Crohn’s disease, psoriasis, and rheumatoid arthritis (RA).1 Infliximab (REMICADE), Adalimumab (HUMIRA), and Etanercept (ENBREL) are three key protein therapeutics, monoclonal antibody or fusion proteins, targeting TNF with reported global sales of almost 30 billion collectively.2 With their broad applicability and impending patent expiry,3 development of bioanalytical methods to accurately measure these biotherapeutics in support of drug development activities is increasing.
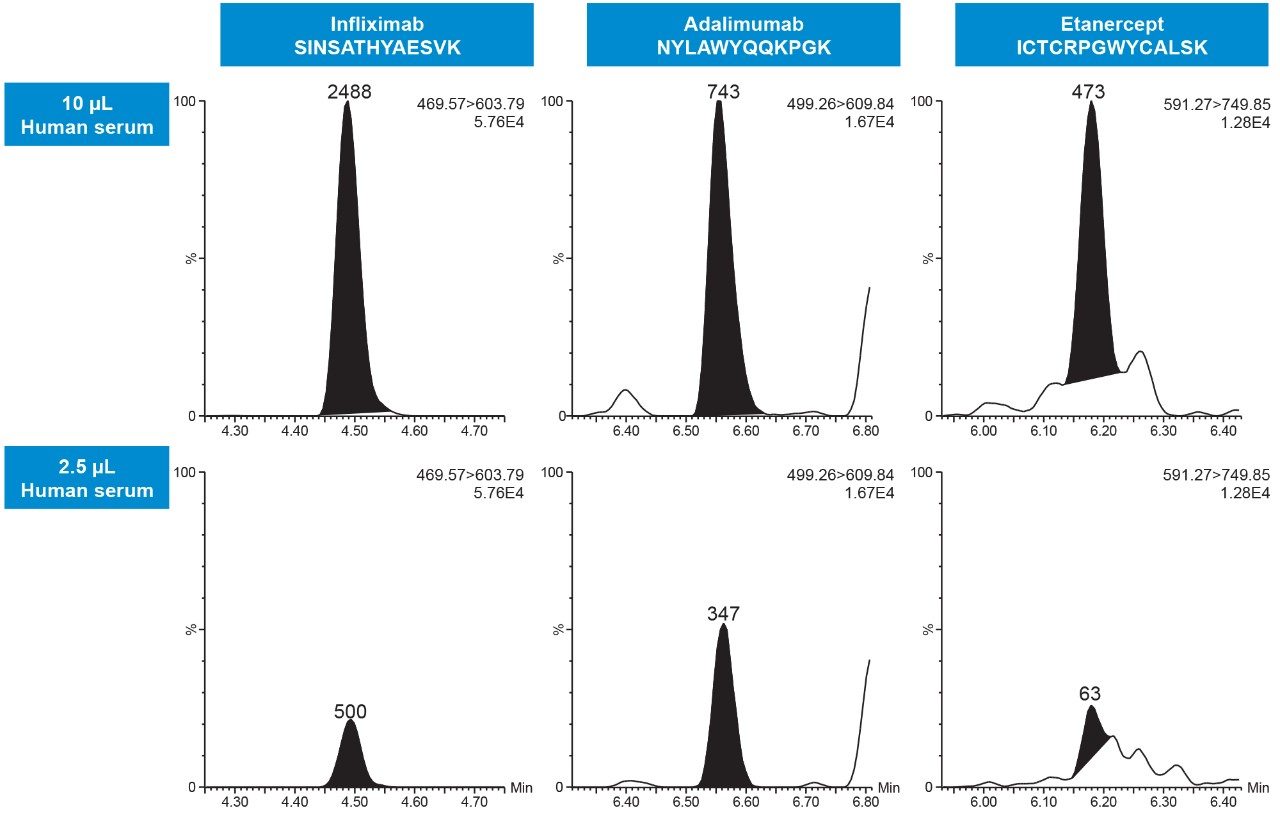
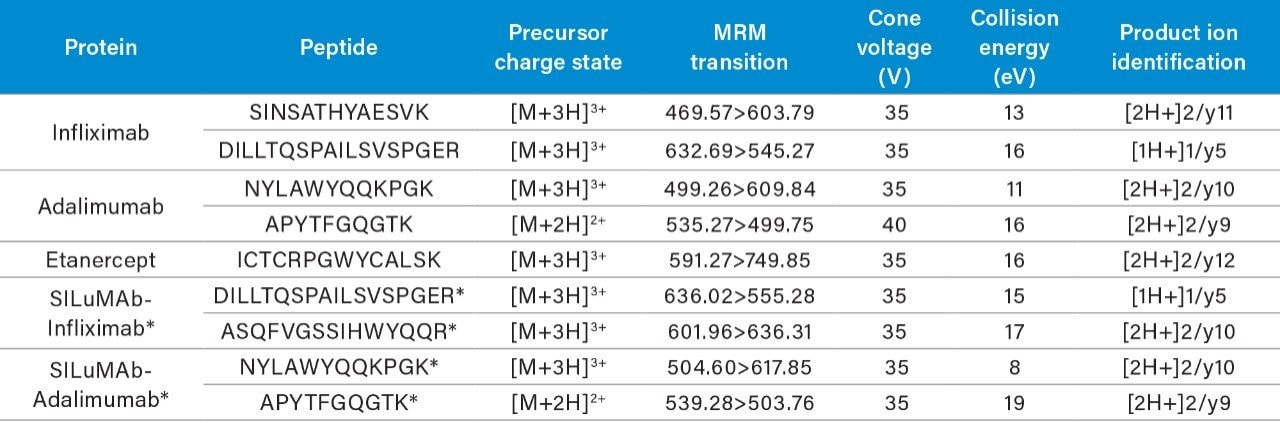
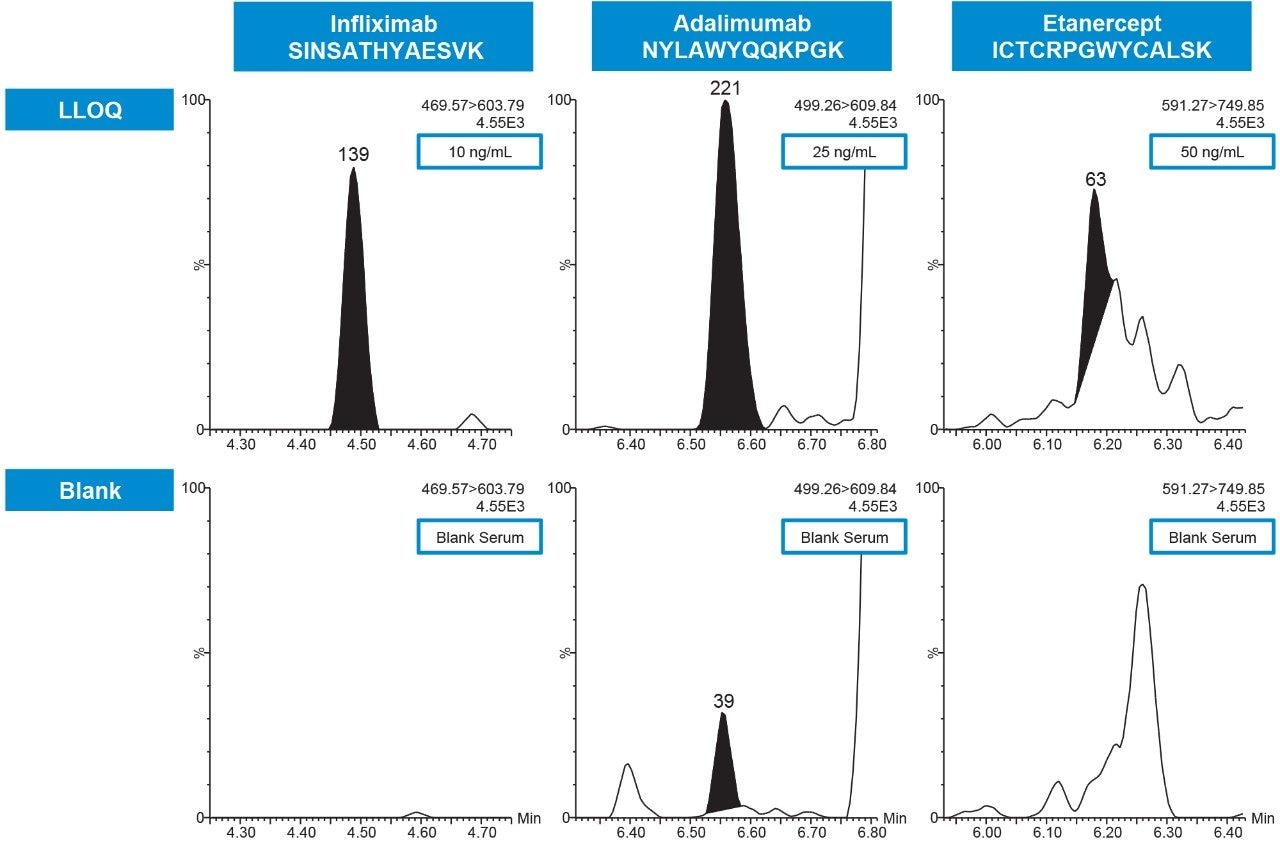
Biotherapeutics have traditionally been quantified via immunoaffinity methods such as ELISA, but these assays can suffer from cross-reactivity and a lack of specificity. However, when the immunoaffinity capture method is coupled to a high specificity detection method, such as LC-MS/MS, the sensitivity and selectivity of the assay can be greatly improved. The most common strategy to prepare proteins for quantitative MS analysis is the surrogate peptide or bottom-up approach, employing enzymatic digestion and subsequent analysis of the resulting peptides. The method described here uses specific immunoaffinity enrichment with target tumor necrosis factor-alpha (TNF-α) followed by a standardized, kit-based approach to protein digestion, and LC-MS/MS detection to quantify ‘free/active mAb’ from ≤10 μL of human serum, achieving lower limits of quantification (LLOQs) of 10–50 ng/mL.