Laboratory developed mass spectrometry assays lack standardization, especially in calibrator value assignment, which contributes to greater interlaboratory imprecision. In this study, we used the MassTrak Immunosuppressants LC-MS assay for tacrolimus TDM, a common LC-MS instrument platform (the ACQUITY TQD), and a proficiency testing survey of laboratories using this assay, to assess whether interlaboratory imprecision could be improved through standardization of LC-MS analysis. Further, we compared the results obtained using this test system to a reference measurement procedure for tacrolimus.
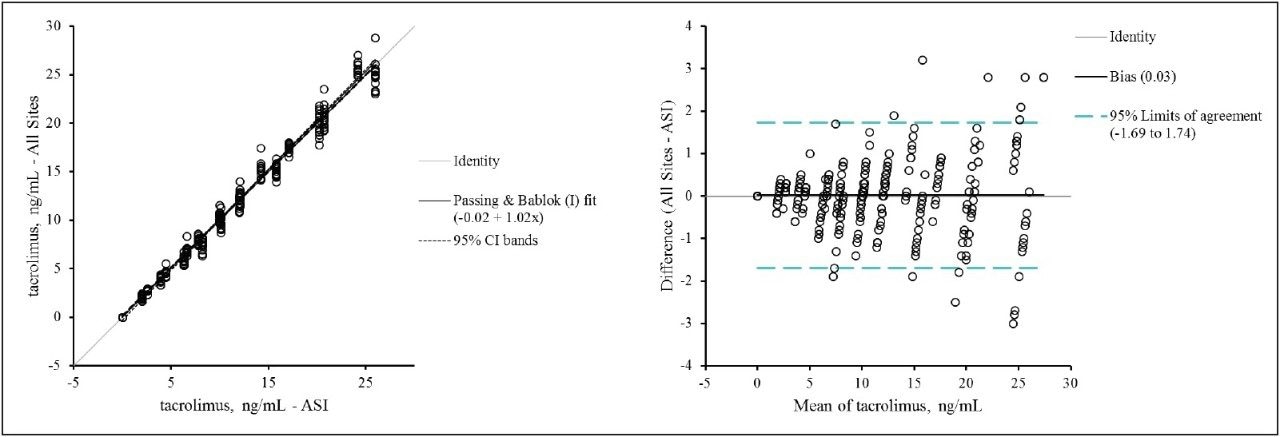
The results of our study demonstrate that the standardization of key analytical variables (calibration materials, sample pretreatment protocols, and chromatography) in the LC-MS analysis of tacrolimus yields highly reproducible tacrolimus measurements across laboratories. This standardization was achieved through the use of the MassTrak Immunosuppressants Kit on a common LC-MS instrument platform. In addition, the MassTrak Immunosuppressants Kit for tacrolimus demonstrated excellent agreement with both a higher-order measurement procedure (ASI) and a reference measurement procedure having a very small measurement uncertainty (LGC). The technique has also been shown to be free from the many factors that negatively impact commercially available immunoassays, namely interference from tacrolimus metabolites,5 hematocrit and serum albumin,6-8 and heterophilic antibodies.9
In summary, while current laboratory developed LC-MS assays may lack optimal interlaboratory accuracy and imprecision, our study demonstrates that improved interlaboratory accuracy and imprecision can be achieved through standardization of the LC-MS analysis with a commercially available LC-MS assay and platform. This level of standardization represents a major improvement over both immunoassays and laboratory-developed LC-MS tests for tacrolimus therapeutic drug monitoring.